





It is often found that religious individuals have better mental health outcomes. In our study, however, we find that praying and participation in religious organizations are associated with more depressive symptoms. Our results do not support the idea that religious behavior, neither public nor private, may be beneficial for the mental health of older Europeans.
Old age can be a time of well-deserved rest with more spare time to spend with family, to engage in social and cultural activities and to enjoy life after all those working years. On the flip side, it is often accompanied with a variety of challenges which are associated with depression: increased dependence, deteriorating health, loneliness and financial difficulties. Therefore, specific research on the social determinants of old age depression is much needed as it leads to a greater understanding in how to improve quality of life in old age. One of such social determinants is religious participation, which is the main focus of our study.
It is often found that religious individuals have better mental health outcomes. Attending religious services and connecting with the religious community can be an important source of social support, while praying might be a way to cope with stress. This way, religiousness can play an important role in improving and protecting old age mental health. However, this relationship could also work the other way around. It might be the case that the positive association between religiousness and mental health simply results from depressed individuals being less likely to attend religious services, and not because religious behavior improves your mental health. In order to take due account of such selection and reverse causality issues, longitudinal data is necessary, as well as a control for previous depression.
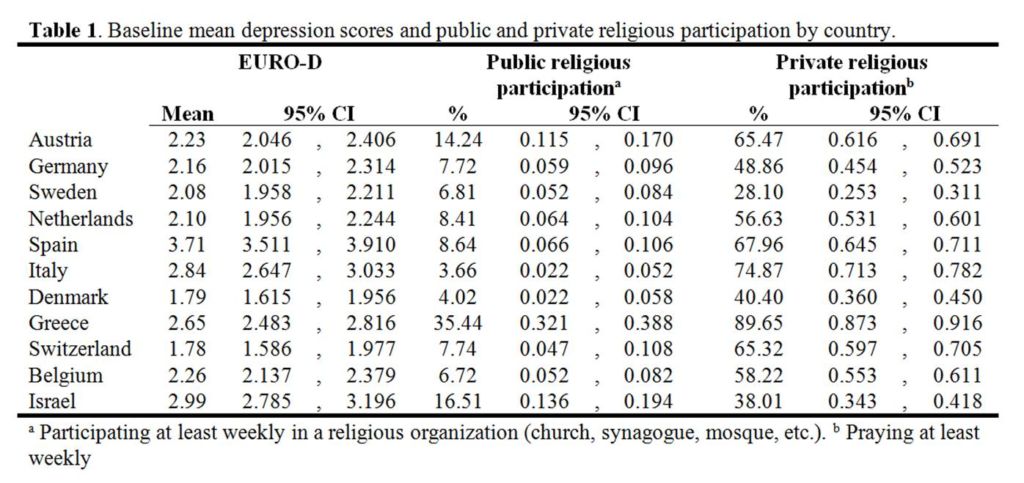
In our article, we assess the association between religiousness and depressive symptoms at old age between 2004 and 2013 for a sample of 7719 individuals aged 65 and older. We use multiple measurements of different aspects of religiousness, including religious service attendance, praying and being religiously educated, and we control for history of depression. First, we look at cross-national differences in religious behavior and depressive symptoms (see table 1). Southern-Europe reports the highest levels of mean depression scores, compared to Northern and Western-Europe. Highest levels of public participation are found in Greece and Israel. Although Italy reported the lowest levels of service attendance, they have one of the highest levels of private religious participation compared to the rest of Europe. Only Greece has a higher proportion of people praying at least weekly, and can be seen as ‘the most religious’ among the 11 countries examined.
In the second part of our study, we look at the longitudinal association between depressive symptoms and religiousness by means of random and fixed-effects models. The results show that religious behavior is associated with depressive symptoms in old age but that the strength and direction of this association is different for public (participating in religious organizations) and private (praying) forms of religious participation (see table 2).
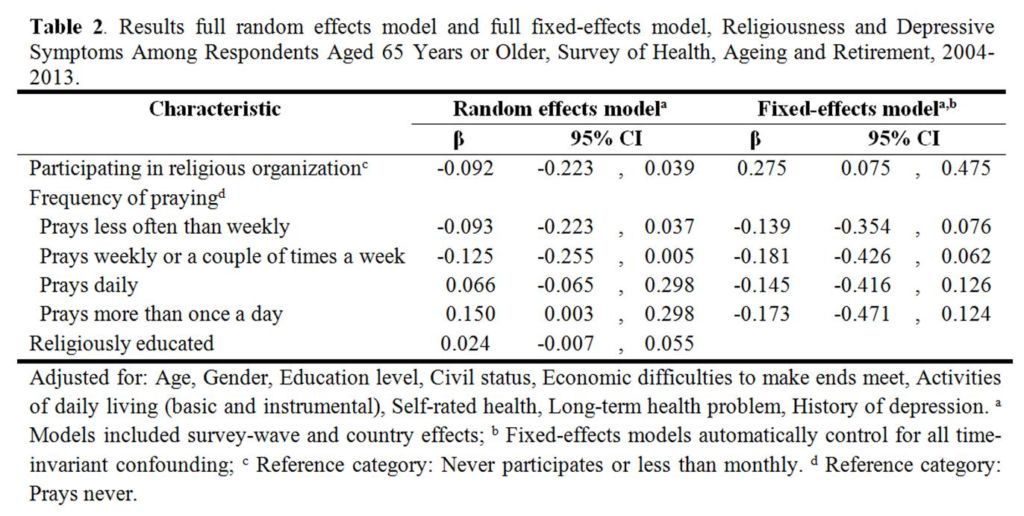
In the random effects model, we find that public religious participation is associated with fewer depressive symptoms. However, this relationship appears to be spurious. Respondents who frequently attend a church service report lower levels of depressive symptoms because they are healthier or have not been depressed in the past. Turning to our fixed-effects model, we find that frequent church attendance predicts higher levels of depressive symptoms. This finding seems counter-intuitive with previous longitudinal research on religiousness and depression in the United States. It might be that in Europe, public religious participation is losing its significance, due to increasing religious individualization. In that case, merely participating in these activities may not be sufficient to benefit from the social support offered by religious organizations. It may be necessary to be a “true believer” or to be “more religious” in order to benefit from religiousness and to internalize religious meanings and values also privately, and not solely by attending religious services.
Focusing on the private aspect of religiosity, we find in the random effects model that praying is associated with more depressive symptoms, even after controlling for several socio-demographic and health controls. Yet, no significant effect is found for praying in the fixed-effects model. The difference between the two models suggests a selection effect: individuals with higher scores on the depression scale are more likely to pray multiple times a day, and continue to do so, compared with less depressed respondents. It is plausible that prolonged reliance on prayer may lead to neglecting professional help, which subsequently leads to rising levels of depressive symptoms. However, we have no evidence that changes in praying behavior are accompanied by changes in the number of depressive symptoms.
Summarized, our findings cannot provide evidence that public policy and healthcare interventions supporting religious behavior, neither public nor private, are effective in reducing depressive symptoms in old age.
About the authors:
Lore Van Herreweghe – Centre for Sociological Research, University of Leuven, Belgium
Wim Van Lancker – Centre for Sociological Research, University of Leuven; Herman Deleeck Centre for Social Policy, University of Antwerp, Belgium
This article is based on: Van Herreweghe L., Van Lancker W. (2019). Is religiousness really helpful to reduce depressive symptoms at old age? A longitudinal study. PLoS One Art.No. e0218557, 1-15.
https://doi.org/10.1371/journal.pone.0218557
Image source: Unsplash, photo by Patrick Fore





Leave A Comment