





Is informal caregiving less detrimental for quality of life when long-term care coverage is more generous? We used SHARE data from Sweden and Denmark and adopted an innovative analytical approach to assess whether this is the case.
It is estimated that approximately 17 percent of the adult population of the European Union provide informal care to relatives, friends or neighbors with care needs at least weekly. A large share of these informal caregivers support ageing parents. Providing care to parents can bring positive things for the daughters and sons engaged in it, such as a sense of purpose or the acquisition of new skills. However, caregiving can also be burdensome and a source of stress. Moreover, caregiving responsibilities may clash with responsibilities in other spheres of life, and the division of care tasks may give rise to tension within families. It is therefore not surprising that research tends to show that the overall impact of caregiving on the health and wellbeing of persons engaged in it is negative.
Almost three decades ago, Pearlin and colleagues developed the caregiver stress model in which they theorized how providing informal care could affect caregivers’ wellbeing and health. In their model, they stressed the role of the context in which care is provided. In contexts where care services are more easily accessible, adult children of older people in need of care are less strongly pushed in caregiver role and they may escape the vicissitudes associated with caregiving. Although the argument that generous long-term care coverage may mitigate the negative impact of informal caregiving on wellbeing is easy enough to follow, it is challenging to test it empirically.
Until the late twentieth century researchers interested in the impact of country level characteristics, such as long-term care coverage, on individuals were frustrated by a lack of cross-national comparative data. This has changed in the last two decades, when several rich, large-scale datasets that allow the assessment of country level differences in individual level outcomes became available. For researchers interested in later life, the most important of these data sources is arguably the Survey of Health, Ageing and Retirement in Europe (SHARE). However, cross-national comparative data, such as SHARE, are by no means a panacea. Most importantly, this is because, unlike treatments in experimental settings, national policies are not randomly assigned. For instance, countries with more generous long-term care coverage also tend to have higher GDP, less traditional gender norms, and weaker norms regarding filial obligations. This has caused many researchers headaches. In many papers using SHARE and other cross-national datasets, scholars have attempted to explain country differences in the impact of an individual level explanatory variable on a particular individual level outcome. Often this is done by estimating so-called cross-level interactions. This means that the effect of the individual level explanatory variable is allowed to vary as a function of a country level characteristic. This approach has also been adopted in various studies of country differences in the impact of informal caregiving on wellbeing outcomes. A schematic overview of this approach is provided in Figure 1.
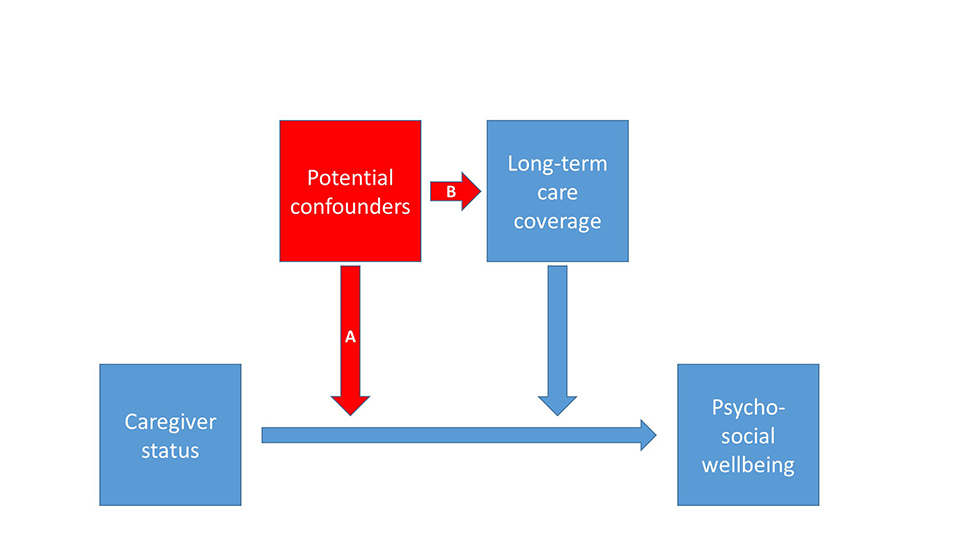
In the approach shown in Figure 1, the effect of caregiving status on the outcome of interest is allowed to vary as a function of long-term care coverage at the country level. Given that this country level characteristic is not randomly assigned, this approach rests on a rather bold assumption, namely the absence of any other country characteristic that both (A) is correlated with long-term care coverage and (B) moderates the impact of caregiver status on the later life outcome of interest. If such so-called confounding variables (shown in red in Figure 1) do exist, then the estimated impact of long-term care coverage on the effects of informal caregiving will be biased. It is difficult to identify all potential confounders, and the relatively low number of countries that are available in SHARE (and other cross-national datasets) limits the number of different cross-level interaction terms that can be included in models simultaneously to adjust for country level confounders. In an attempt to provide more conclusive evidence on the way long-term coverage shaped the impact of caregiving on quality of life, we adopted a somewhat different approach. We focused specifically on Sweden and Denmark and exploited the fact that, at the time we conducted our analyses, six waves of SHARE data that covered the period 2004-2015 were available. Over this period, notable changes in long-term care coverage occurred. Around the turn of the century, long-term care coverage was clearly more generous in Denmark than in Sweden. However, since approximately 2008 notable cutbacks in long-term care coverage took place in Denmark, but not in Sweden. Consequently, the difference between both countries in long-term care coverage was smaller in the period 2011-2015 when the SHARE data collection for waves 4-6 took place than in the period 2004-2007 when SHARE waves 1 and 2 were collected. This enabled us to assess how long-term care coverage shaped the impact of informal caregiving on quality of life with an extended difference-in-difference approach, or, if you will, a “difference-in-difference-in-difference” approach. This means that we tested whether a reduction of the difference between Sweden and Denmark in the impact of caregiving on quality of life took place between the 2004-2007 period and the 2011-2015 period when long-term care coverage in both countries became more alike. A schematic presentation of our approach is presented in Figure 2.
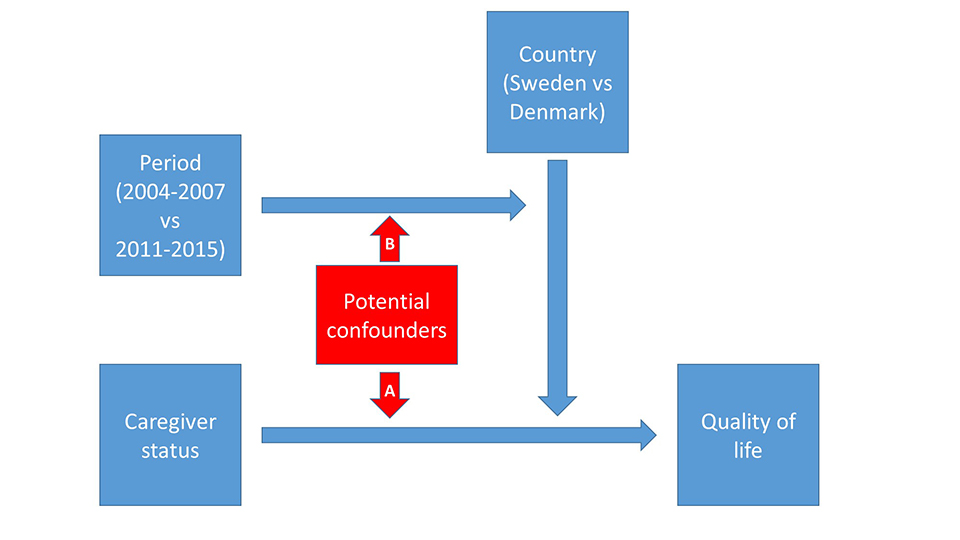
Although the approach presented in Figure 2 still leaves room for confounding, the underlying assumptions are weaker than those in the commonly used approach presented in Figure 1. This is because arrow B in Figure 2 is much more specific than arrow B in Figure 1. In our approach it is a necessary condition for confounders have developed differently in Sweden and Denmark over the considered time-frame. This means that, unlike in the conventional approach, unobserved but stable differences between countries, for instance on policy, cultural or economic dimensions, cannot bias our estimate of the moderating effect of long-term care coverage on the impact of caregiving on quality of life.
Our analyses showed that the difference between Sweden and Denmark in the impact of informal caregiving on quality of life became smaller when long-term care coverage convergence took place between both countries. Given the relatively weak assumptions underlying our approach, our results thus strongly suggest that caregiving has a less detrimental impact on quality of life when long-term care coverage is more generous.
About the authors:

Dr. Thijs van den Broek is assistant professor Socio-Medical Sciences at Erasmus School of Health Policy & Management, Erasmus University Rotterdam (The Netherlands).

Prof. dr. Emily Grundy is Professor of Population Science and Director of Institute for Social and Economic Research (ISER) at the University of Essex, Colchester (United Kingdom).
The article is based on:
Van den Broek, T. & Grundy, E. (2018). Does long-term care coverage shape the impact of informal care-giving on quality of life? A difference-in-difference approach. Ageing & Society. https://doi.org/10.1017/S0144686X18001708
The research leading to these results has received funding from the European Research Council under the European Union’s Seventh Framework Programme (FP7/2007–2013)/ ERC grant agreement n° 324055.




Leave A Comment