





Depression is common in later life. Several instruments have been developed to detect the presence of certain symptoms or emotional disorders, based on cut-off points. However, the use of a cut-off does not allow identification of depression sub-types or distinguish between mild and severe depression. Our work aims to apply a model-driven approach to classify individuals into distinct sub-groups, based on different combinations of depressive and emotional conditions.
Depression is one of the most common mental disorders affecting older people, which often coexists with other medical illnesses and physical disabilities. Higher prevalence of depression among women than men is well documented and persists also during later life. People with depressive symptomatology are at higher risk of mortality.
Later-life depression is characterised by a large heterogeneity in symptoms. The identification of substantial and meaningful sub-groups of depressive symptom profiles has important implications for research, public health policies and clinical practice. Indeed, the public health burden of depressive symptoms in older adults is expected to increase rapidly, given the large proportion of people in this group.
Several screening tools are available for detecting such disorder, and can be divided in two broad sets of instruments: the first is designed to collect information on symptoms, conditions or signs that best reflect diagnoses of mental disorders (i.e., the Diagnostic Interview Schedule or the Composite International Diagnostic Interview). The second is designed to measure more generic factors (psychological distress), collecting the presence of certain symptoms or emotional disorders, such as the Centre for Epidemiologic Study Depression Scale, the Beck Depression Inventory and the EURO-D.
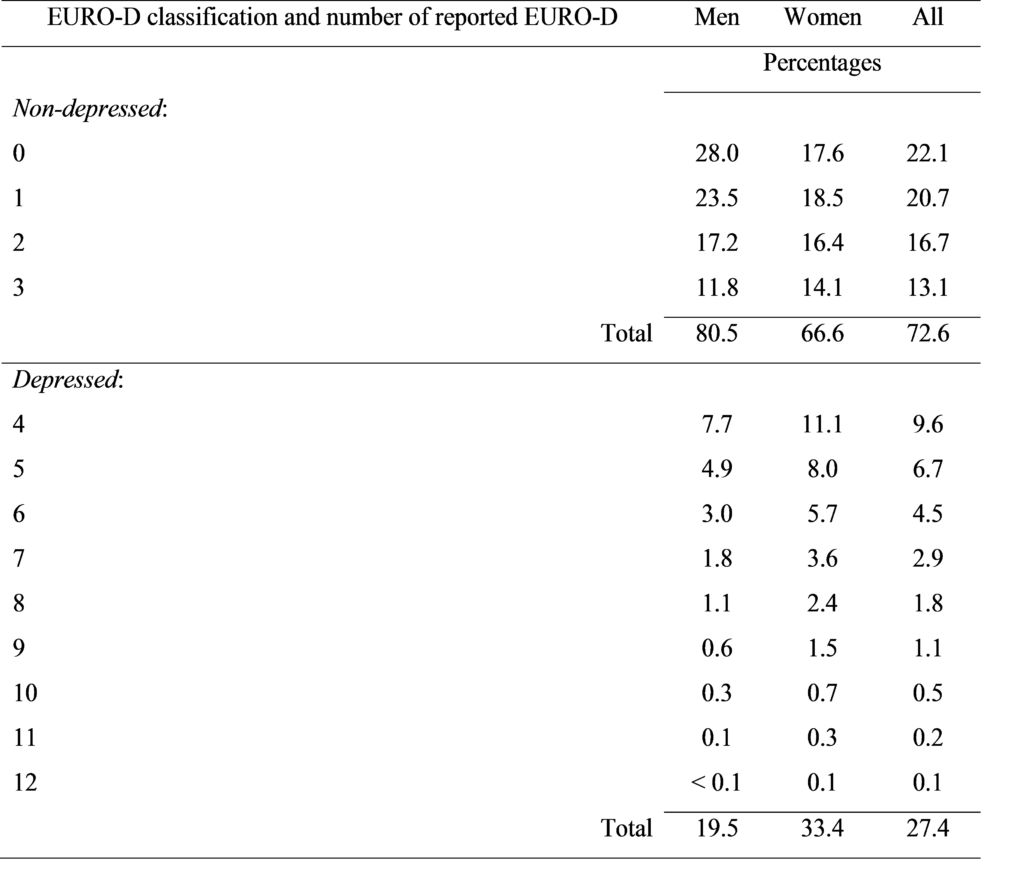
The EURO-D is a depression scale that was developed and validated by the EURODEP Concerted Action Programme. The scale includes 12 items: depression, pessimism, wishing death, guilt, sleep, interest, irritability, appetite, fatigue, concentration, enjoyment and tearfulness. It is a symptom-oriented scale, that is it identifies the presence or not of some depressive or emotional manifestations: its score ranges from 0 (the lowest level of depression) to 12 (the highest level), but it does not provide diagnoses of any mental disorders. Depressed individuals are identified with a EURO-D score greater than 3.
Although widely used, a cut-off to identify people at risk of depression does not discriminate among depression sub-types nor between mild and severe depression: older people may differentiate from younger population for the combinations of symptoms that characterise their mental disorders. We believe that a more accurate classification (according to the number and type of the reported items) than the simple dichotomisation ‘depressed’ versus ‘non-depressed’ may be more helpful to researchers, clinicians and clinical investigators. To this aim, we introduced an alternative approach to identify meaningful sub-groups of homogeneous depressive symptom profiles among such population. Our approach is based on two different statistical solutions – Latent Class analysis and Factor Analysis – to classify individuals with different patterns of depressive disorders. Individuals are grouped according to the likelihood of observing certain patterns of reported items. This solution is applied to data collected by the EURO-D scale in the sixth wave of the Survey of Health, Ageing and Retirement in Europe (SHARE), carried out in 2015.
Results in Table 1 show that 27% of respondents (20% of men and 33% of women) report being depressed according to the EURO-D scale. Looking at the combinations of the reported symptoms, the majority of the depressed people indicate four or five items, and only a small proportion of them (for women it is larger than 7.5%) report nine or more symptoms.
Using our technique, we classify people in seven categories of depressive and emotional problems: very low risk of depression, low risk of depression, middle risk of depression, high risk of depression, depressed, severely depressed and extremely depressed (Table 2).
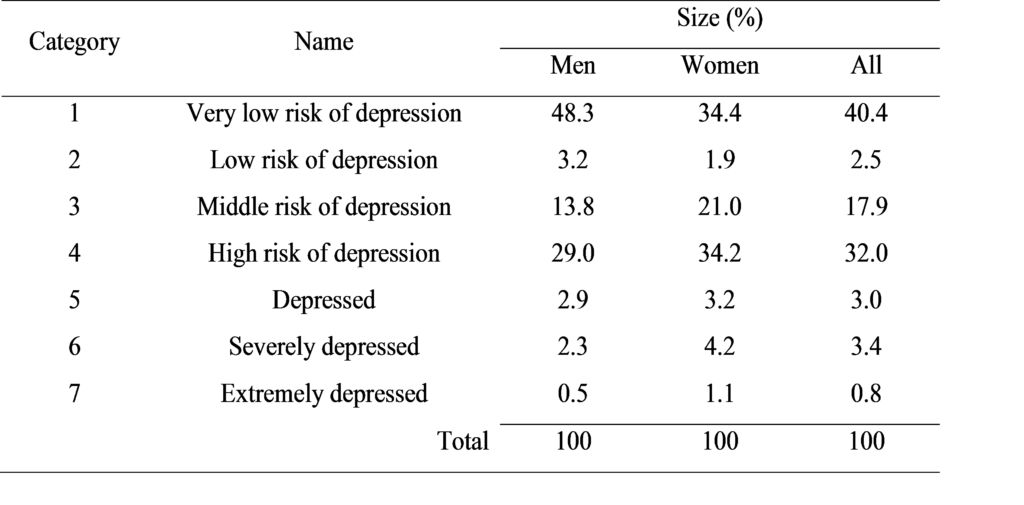
According to our taxonomy, about 40 per cent of the total population is classified at a very low risk of depression. Individuals in this cluster present a similar pattern or combination of such symptoms (i.e. no or just one or two reported items). The first two categories (very low risk of depression and low risk of depression) are mainly composed by men.
The last three categories (depressed, severely depressed and extremely depressed) are characterised by individuals with a high probability of reporting several depressive and emotional problems. It is likely that in such cases depression corresponds to a clinical diagnosis.
One-third of respondents fall into the high risk of depression category, which is mainly composed of unhealthy respondents (for instance almost 60% of them report two or more chronic diseases) and women (more than 60%): these individuals are not yet classified as depressed, but should be monitored to prevent future development of depression.
The main strength of our approach is the identification of several levels of severity of depressive disorders, that goes beyond the simple dichotomization “having” or “not having” depression (present or not). This solution allows flexibility in labelling each category that was obtained, according to the nature, type and number of the mental disorders under investigation. Yet, this approach can be easily applied to data collected by any depression instrument designed to detect the presence of certain symptoms or emotional disorders. We have limited our approach to cross-sectional data for the sake of clarity. However, given the dynamic nature of depression, this approach could be extended to model developmental trajectories or patterns of changes over time.
These clusters are characterised by different and interesting mixes of symptoms and these differentiations may help epidemiologists, clinicians and health researchers to better observe and understand the presence and the severity of any manifestations of depression among older adults; this refined classification may provide the basis for improving current protocols for detecting different levels of depressive disorders and helping to develop customised intervention and treatment programmes.
About the authors:
Chiara Gennaro, Palladio Group S.p.A., Dueville, Italy
Omar Paccagnella, Department of Statistical Sciences, University of Padua, Padua, Italy
Paola Zaninotto, Department of Epidemiology and Public Health, University College London, London, UK
The article is based on:
Gennaro, C., Paccagnella, O., & Zaninotto, P. (2019). A model-driven approach to better identify older people at risk of depression. Ageing and Society, 1-23. doi: 10.1017/S0144686X19001077





Leave A Comment