





Old-age pension in Denmark is among the highest in the world although life expectancy lags behind that of many other welfare states. The Danish pension age is adjusted in line with the projected increase in life expectancy without taking social differentials in mortality into account. Neither does the decided increase in retirement age take social differentials in expected lifetime in good health into account. The purpose of the study was to investigate occupational disparities in partial life expectancy and expected lifetime in good/poor health between age 50 and 75.
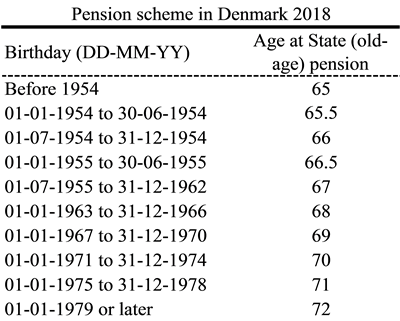
The Danish response to the demographic challenge of the ageing population is to adjust the old-age pension in line with projections of increasing life expectancy. As shown in the pension scheme table below, the retirement age is planned to increase from 65 years to 72 years for those born in 1979 or later. The social democratic government in Denmark was elected in 2019 on a promise to introduce a flexible retirement age taking social differentials in mortality into account.
Life expectancy is an aggregated indicator that blurs important details in the mortality pattern changes when looking at trends and projections. This has been illustrated clearly in a Danish study of socially disparate trends in the distribution of age at death (https://bmjopen.bmj.com/content/7/5/e014489). Significantly different changes in lifespan variation between socioeconomic groups were seen in the age range around retirement age. Another important element for considering a flexible pension scheme is expected lifetime in good health, which differs between socioeconomic positions.
We estimated occupational disparities in partial life expectancy and health expectancy (lifetime in a specific health state) between the ages of 50 and 75 using Danish national register data on occupation and mortality and self-reported health data from the Danish part of The Survey of Health, Ageing and Retirement in Europe (SHARE).
The International Standard Classification of Occupations (ISCO) was used to divide occupation into the four groups:
Low skilled blue collar: Elementary occupations; Plant and machine operators and assemblers;
High skilled blue collar: Craft and related trades workers; Skilled agricultural and fishery workers;
Low skilled white collar: Service workers and shop and market sales workers; Clerks;
High skilled white collar: Technicians and associate professionals; Professionals; Legislators, senior officials and managers.
Because the Danish SHARE panel was linked to registers (http://www.share-project.org/special-data-sets/record-linkage-project/reglink-sharedk.html), we achieved the same data source to identify the present or latest held occupation for SHARE participants when combining health and mortality by occupational group. Thus, information on occupation was from registers, while health status was self-reported from SHARE.
To construct occupational-specific life tables we calculated age-specific death rates by occupational group by linking register data on occupation and mortality for the complete Danish population aged 50-75 in the period 2011-15.
We used cross-sectional data from the fifth wave of the Danish SHARE survey conducted in 2013-14 and additionally included respondents who participated in the fourth wave from 2010-11 but were missing in the 2013-14 data collection. The final study sample included 3179 respondents between age 50 and 75. Information on respondents’ occupation from register data was linked to SHARE by use of the unique personal identification code assigned to all citizens. Activity limitations was measured using the question “For the past six months at least, to what extent have you been limited because of a health problem in activities people usually do?” and respondents were coded as being limited if they answered “severely limited” or “limited, but not severely”. Long-term illness was measured asking respondents: “Some people suffer from chronic or long-term health problems. By chronic or long-term we mean it has troubled you over a period of time or is likely to affect you over a period of time. Do you have any such health problems, illness, disability or infirmity?” with answer categories “yes” or “no”.
Data from the occupation-specific life tables were combined with data on prevalence of activity limitations and long-term illness by occupation from SHARE to estimate health expectancy by standard demographic methods as suggested by Daniel F. Sullivan in 1971.
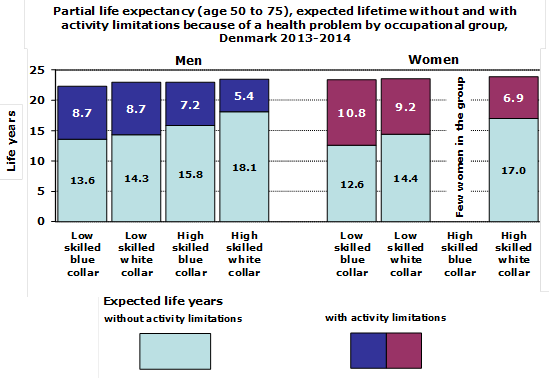
Results for activity limitations are shown in the graph below. From the graph it appears that although social disparity in partial life expectancy was modest due to low mortality in the ages between 50 and 75 the social gradient in expected lifetime without activity limitations was significant. Thus, expected lifetime from age 50 to 75 differed by 1.2 years between high skilled white collar and low skilled blue collar males, whereas years without activity limitations differed by 4.5 years in favour of high skilled white collar males. The difference in partial life expectancy between women in high skilled white collar and low skilled blue collar occupations was 0.5 years whereas the difference in expected years without activity limitations was 4.4 years. It also appears, that women could expect fewer years without limitations than men despite more years of total life (between age 50 and 75).
In addition, results for long-term illness also demonstrated a clear social gradient. Thus, the difference in expected lifetime without long-term illness between high skilled white collar and low skilled blue collar occupation groups was 3.8 years for men and 4.1 years for women (in favour of high skilled white collar occupations).
The study confirms persisting social inequality in health in Denmark and the results indicate that implementing the same age of retirement for all will in practise lead to social inequality between occupational groups not only in the number of retirement years but also in the number of retirement years in good health.
About the authors:
Henrik Brønnum-Hansen, Faculty of Health Sciences, Department of Public Health, University of Copenhagen, Denmark
Else Foverskov, Faculty of Health Sciences, Department of Public Health, University of Copenhagen, Denmark
Ingelise Andersen, Faculty of Health Sciences, Department of Public Health, University of Copenhagen, Denmark
This article is based on:
Brønnum-Hansen H, Foverskov E, Andersen I. Occupational inequality in health expectancy in Denmark. Scandinavian Journal of Public Health, 2020, https://doi.org/10.1177/1403494819882138





Leave A Comment